Category Archives: Lean Healthcare w Polsce
Lean healthcare – the first project accomplished in Poland
How to manage processes in a hospital and other medical facilities? So many variables affect realization of medical services that it is not a simple matter at all. Lean healthcare is about clinical processes optimization. Substantial services makes it impossible to be objectively evaluated. The most difficult aspect is its impermanence that inspires to search for new solutions, tools and variations, in order to keep all services on the same good or better quality level. It isn’t so simple to describe a process and maintain these certain practices. Everyone aim for a kind of established standard, meaning the best current accessible technique and manner of performance abide by medical personnel. Universal solutions are result of everyday situations and aren’t good for client, namely the patient. Each physician, nurse or other member of medical personnel have their unique knowledge and experience which create different approaches to maintain into one process scheme. Simplicity of rules listed on a „paper” but in reality it may confront many aberrations and exceptions. Lean healthcare is geared towards both, efficient, lean services provision and useful tools and techniques to unify clinical process. Patients and personnel safety are number one priority.
Aims of lean healthcare
Lean healthcare philosophy includes set of precise tool and methods to optimize patient flow in clinical process, remove barriers and gaps causing errors and delays (losses and waste). Set of tools based on lean manufacturing is becoming more and more numerous. In order to improve any clinical process it is important to define its purpose, issues and obstacles faced by the personnel during every day work. Each hospital, it’s department or clinic differ a lot from each other by their infrastructure, use of disposable materials and reusable utilities, medical equipment and medications. While implementing lean healthcare philosophy it is crucial to consider the specificity of a department. Not always the beneficial result from other department will work out for other clinic.
First practical use in Poland
Success of implementing lean hospitals is conditional to the target place but above all the people that work in it. Medical specialists, nurses, medical care assistants, technicians and all other parts of the personnel not only shall accomplish their tasks with all obligatory duties, present knowledge and internal procedures but also with an ability of operational communication. Soft skills play a significant role of medical personnel cooperation based on personnel-patient and personnel-personnel relations. Training does’t assure these essential skills so here is the point where professional practice and positive approach to a patient matters. Lean healthcare tools are to simplify communication, fill any gaps and enhance information accessibility. Best solution for above given problems may be 5S methodology, worksite organization, visual board and visual management.
Tools of this kind are very useful on critical sites where an error may result with patients death or his severe complications e.g. integrated operating theatre. Proper infrastructure will optimize flow of medical equipment, utilities and the patient itself as a whole process. In order to achieve a legitimate optimization it is essential to map the process (use of VSM – visual stream mapping), identify every step of given process, define number of involved personnel, set intervals around all activities and define time consumption of each step. The result is a valid process map which will be helpful to design a future state map. One of lean tools called the spaghetti diagram can reduce distance made by personnel, its fatigue and increase availability towards patients. The results will present all most common paths used by personnel and later improvements may be implemented in accordance with the outcome paths. Another lean healthcare tool called Kaizen works as an application and suggestion system for personnel to submit any remarks, observations or inspirations to enhance any process. The first project implemented in Poland was about implementing visual management, medical and clinical process optimization and communication improvement of medical personnel. Project had been awarded by worlds experts of lean management at Lean Enterprise Institute and has won the second prize as the best lean management implementation in Polish services sector. Katarzyna Zlotowska as the head of the award-winning project leads several projects in hospitals across Poland. The results are available on Lean Hospitals website containing knowledge base concentrated on lean healthcare and quality.
Lean healthcare benefits
In conclusion, lean healthcare in health services is one big innovation on a world scale and its results are measurable and surprisingly positive. Here are some advantages after implementing several tools and methods of lean hospitals in a medical entity:
- more than 60 000 zl lower costs of functioning process
- 90% less accidents
- 30% reduction of medical materials, drugs and equipment
- 20% better patients satisfaction and communication improvement
Each unit is composed of processes to be improved. Despite the fact that lean healthcare is a specific use of universal tools and solutions, the process-based approach and patient flow in a process are very convenient to use as well as easy to examine. Both are to create value added.
Lean tools used in Healthcare
Healthcare is an essential component of the economy that aims not only at healing people, but also cooperating with research entities and striving to adopt innovative solutions. Hospital is an institution that provides a patient with medical treatment by specialist staff and with the use of the specialist equipment. A patient should never disrupt the functioning of the organization. Both infrastructure and processes taking place in hospital should be organized in such a way that a patient, being the most important person, can smoothly, consciously and without unnecessary waiting go through the whole medication, as a partner and co-decision maker together with the doctor. Just as the surgeon in the operating room is equipped with a toolbox containing forceps, scissors, surgical blades, bum bag as well as a team of specialists, including an anesthesiologist, nurse, and a circulating nurse, that are needed to carry out an operation on a patient, the manager that manages the processes taking place in a medical facility and is responsible for quality also needs the “toolbox” allowing them to analyze the clinical processes, effectively manage resources and eliminate bottlenecks and other problems. There is increasing talk of the efficient flow with respect to the services rather than manufacturing industry exclusively, in the case of which a car might be such an element, whereas in healthcare facility it is a patient. Patient, being an “element” of the flow process, is treated in various ways from the need-disease diagnosis to the moment it is satisfied, which means that the patient has recovered or their state of health has improved. Lean healthcare aims at generating adding value for a patient, by shortening the time of patient’s “journey” and increasing patient’s safety. The more efficient the flow is, the more effective the use of resources is, for instance when a patient makes an appointment with a medical specialist, be it a diabetes specialist, and has to wait 10 days (240h) for a visit, and the visit itself lasts 30 minutes (0.5h), the efficiency of the process equals 0.5/240=0.2%. This is the only part of the whole process that contributed to the patient’s awareness of their health conditions and choosing the right therapy, all the rest was useless. So how can we organize the process so that its efficient flow rate is high? We should eliminate bottlenecks and places, in which no added value is generated, and avoid waste. Lean healthcare tools are needed in healthcare processes for treatment to be successful and resources to be effectively used. What tools do they comprise?
Flowcharts for clinical processes
A process consists of a variety of activities that transform data inputs into data outputs. Each medical facility should identify the clinical processes, which are the processes in which a patient is directly involved. Doctors act in accordance with the current medical knowledge, legal requirements and their own experience; requirements and experiences of all the process participants should be gathered in order to define one standard for a process. Defining labor standard is connected with choosing the most effective way of implementing the clinical process. The objective is not to introduce strict patterns of behavior but rather to define the line of action that would enhance the safety and quality level. Defining what kind of processes take place in a given facility (and the boundaries of these processes) is not easy; what is known are the procedures and the delivered services (payments between the Payer and service providers specialists are responsible for that). It is more difficult to define them in multi-specialist hospitals that consist of 40 various departments rather than a small FP clinic. It is worth to answer the questions below:
- What are the patient’s medical problems that made them visit our clinic?
- What kind of activities are we going to perform in order to satisfy our clients and meet their requirements?
- What kind of services do we provide to the patients with similar problems and medical diagnosis?
- Which services are provided most frequently or which services constitute the most important part of the organization?
Answering the questions above will allow us to choose the major processes that take place in a department, in a medical facility. Upon getting informed on the process, it is worth to list all the stages it comprises and activities that are performed. Remember that it is a patient that initiates the process (they ask for a particular service) and terminates it. As far as activities are concerned, it should be established which people are responsible for performing them and providing vital documents, blank forms and tools. Creating a flowchart requires from its author the use of particular shapes-graphics, the most important of which is so called a decision point. On the one hand it is very often a critical point in the whole process, but on the other hand it divides the process into two different patterns of actions. Visualization of the process is not the objective itself, a flowchart is located in the places where the services are delivered, for instance in a nephrologist’s office. Despite being aware of the procedures, each doctor may perform the same treatment in a different way; standardization fosters increased safety of a patient during the process, improvement of the flow and elimination of errors and risks that might occur. The risk of committing a mistake, omitting an important step in the process or forgetting to fill the medical documentation is substantially smaller when the medical staff abides by the flowchart (there always occur some deviations that depend on patient’s health conditions). This solution has been widely approved by the medical workers, who are involved in making necessary adjustments whenever the law, requirements or the process itself changes.
Visual management: color scheme, andon, safety cross
The picture is able to convey the message much more effectively than words. Visual management aims at optimizing clinical processes and specifying the further treatment in the process. VM is composed of light and sound signals, pictures and graphics, which allow us to monitor the process and respond immediately in case of any disturbance, evaluate the current state and compare it with the desired state – the one that is planned. VM facilitates the work of medical staff by indicating critical situations. The example of VM application can be found in a clear separation between the “soiled” and clean working areas in the operating room that is indicated by different floor colors. Blue color stands for the sterile area, whereas non-sterile places are characterized by the red color of the floor (soiled locker room, soiled warehouse, utility room);
- sound information (andon) regarding incorrect parameters during the process of hemodialysis in the form of an audible alarm and a red lamp (a flashing alarm)
- daily analysis of incompatibilities: undesirable events, medical incidents and situations which potentially may be a source of accidents are marked on a board called the LeanCross – a safety cross. Everyday situation on the ward is assessed on the board – if there was an accident or a dangerous situation on the given day or perhaps the day was peaceful, without any accidents.
3. 5S Method
The aim is to create an organized workplace which will allow for reducing the number of errors and the amount of resources used as well as facilitating the flow of values during a process. The task is to make possible constant work basing on the same principles as well as to allow for the introduction of improvements. The method comprises 5 steps which are systematically assessed and analyzed. It is a constant process of maintaining order and assessment of a workplace that uses instruments of visual management allowing for solving problems, such as:
- searching for medical instruments, materials, medicines which are urgently needed;
- lacking medicines and other materials that are quickly used up;
- excessive moving from one room, ward or building to another, which not only exhausts the staff but also leads to an increased number of errors made;
- lack of space needed for the realization of a process;
- disorder, keeping the materials needed in the rooms most distant from the place of the realization of a service.
An effective implementation of the 5S method allows for reducing or eliminating the wastage occurring in a clinical process.
4. FMEA risk analysis in the clinical processes
It is a new use of an instrument, known from the sixties of the twentieth century, which serves to predict causes and consequences of potential errors. According to the rule “prevention is better than cure”, the best proactive way to eliminate or minimize the clinical risk is a constant analysis of a process. FMEA, the analysis of causes and consequences of potential flaws, allows for predicting errors which may occur in the process and taking actions to prevent them, instead of introducing corrective measures after the error has occurred. If we familiarize ourselves with the process well, conduct an analysis of every activity it comprises, gather specialists’ opinions (the interdisciplinary team for the FMEA analysis), we may predict errors and design a process in such a way that in the next few years no significant risk will occur. FMEA is employed not only to design new processes but also for the existing ones. The improvement of quality depends to a great extent on the management, culture and possibility of creative thinking rather than on the implementation of specific methods and instruments (M. Graban). This is why employing only a method, without persons involved in a process (physicians, technicians, unlicensed assistive personnel, registered nurses) and without brainstorming conducted preferably in the GEMBA – the place where the medical service is realized, will not be effective but short-lived. The most important steps during the analysis are:
- To determine possible problems which may occur, basing also on historical data.
- To investigate if these problems have a great influence on the life and health of the patient.
- To define in what ways we may detect the error.
It should be remembered that after every interference in the process, after every change in the procedures, after using new resources another analysis should be conducted and the risk reassessed.
5. Kaizen
How to optimize a process in an easy and money-saving way, appreciating the staff at the same time? Introduce the Kaizen card – a form where an employee notes down propositions of an optimization of a process. These may regard redesigning of the process, a change in the system of infrastructure, a purchase of only a minor instrument or organization of a meeting to discuss the current problems, to analyze them and to detect the root cause of their occurrence. The added value is not only ideas of employees but the fact that they are involved and want to have influence on the process they participate in.
The most frequently optimized areas are:
- the hospital warehouse of medicines, equipment and single-use materials
- areas concerning the care of the patient
- treatment rooms
- transportation of the sick
- bedlinen management
6. Error analysis using 5Why and Ishikawa diagram
In a medical facility every day there occur situations which have a negative influence on the patient’s health. They may be prevented by analyzing the root causes of the occurrence of the error. Why? The sole correction of the error will erase it but will not be a warrant that it will not occur any more. This is why the source-factor which caused the flaw must be identified. Sometimes there are many causes which regard various areas. Ishikawa diagram divides these causes into groups and allows for defining visually which group had the greatest influence on the occurrence of the problem. When conducting an analysis with Ishikawa diagram we use also the 5Why method. We ask a question, the answer for which is another question.
To conclude, in the article there were presented some of many instruments and methods used in healthcare facilities in Poland and in the world. The type of the method depends on the scale of a facility, the vision of the management, the staff’s involvement and the resources available. The use of lean healthcare instruments in order to optimize clinical processes is an example that management innovations have a positive influence on the healthcare sector. We should remember that the way to achieve positive results is not simple nor fast. The medical staff has to adapt to new rules. This is achieved more easily by implementing lean “with small steps”, gradually. If the staff sees the sense and potential in using a new procedure, if they even demand more maps of a process (the mapping of clinical processes technique), we may proceed with the next stage and name specific instruments without scaring the employees off.
Six sigma in health care
Czym jest six sigma i jak ją wykorzystać w ochronie zdrowia? Jest to metoda poprawy, duże działanie usprawniające, które ma przełomowy charakter. Projekt taki rozpoczyna się w krytycznym obszarze firmy, w celu osiągnięcia oszczędności, zwiększenia konkurencyjności firmy. Kto był pierwszy? Po raz pierwszy metodę SIX SIGMA wykorzystała Motorola w latach 80 XX wieku. Czym różni się six sigma od lean management? Six sigma ma za zadanie przede wszystkim rozwiązywać problemy biznesowe, a lean ma eliminować marnotrawstwo.
Analiza problemu – six sigma
W celu pozytywnie zakończonego projektu ważne jest wybranie nie tylko problemu, który odpowiada metodyce six sigma, lecz również stosowanie metody DMAIC (define, measure, analyze, improve, control). Po określeniu procesu, w którym występuje problem należy go dokładnie prześledzić, zrozumieć i zebrać jak najwięcej liczb i danych. To na nich opieramy analizy statystyczne, wyciągamy wnioski i wdrażamy zmiany i usprawnienia. Każdy etap to szereg działań wykorzystujących wiele narzędzi między innymi takich jak: burza mózgów, metody statystyczne, mapowanie procesów klinicznych, 5why, 5W2H, analiza Pareto, diagram Ishikawy, standardy, zarządzanie wizualne, komunikację interpersonalną, zarządzanie czasem. Czy w ochronie zdrowia problem również nie może mieć znanego rozwiązania?Więcej już niedługo…
Zyski i koszty wdrożenia rozwiązań lean hospitals
Wstęp
Praca nad case study o kosztach związanych z lean healthcare rozpoczęła się w grudniu 2015. Na podstawie artykułu opublikowanego przez ASQ dotyczącego zarządzania wizualnego, pt.:” Polish Dialysis Center Employees Use Visual Management to Increase Safety, Improve Organization of Medical Facility” napisanego przez Katarzynę Złotowską i Adam Wise. Na podstawie informacji z opisu wdrożenia zarządzania wizualnego w Regionalnym Centrum Nefrologii rozpoczęto współpracę z Douglas Wood, który jest ekspertem w dziedzinie kosztów jakości. Poniższy artykuł przedstawia koszty jakie poniesiono oraz zyski, jakie osiągnięto poprzez wdrożenie narzędzi lean healthcare w tej placówce medycznej.
Jak inżynier poprawił bezpieczeństwo w szpitalu?
Regionalne Centrum Nefrologii (RCN) to jednostka (szpital) specjalizująca się w opiece nad pacjentami z przewlekłą chorobą nerek, w której zachodzą procesy wzajemnie się uzupełniające, koniec jednego jest początkiem dla kolejnego procesu. Dla pacjenta ważna jest wizyta u specjalisty (wartość dodana) i jak najkrótszy czas oczekiwania. Mało który pacjent jest świadomy tego, że wszystkie usługi medyczne to procesy, na które składa się wiele zmiennych. Jak je zorganizować by były realizowane w optymalny sposób? Zastosować filozofię lean management, lean healthcare.
Podróż z Leanem rozpoczęła się od systemów jakości, najpierw od ISO 9001, które RCN utrzymywało od kilku lat. Szczególnie przy wdrażaniu kolejnego systemu PN-EN 15224 zauważono potrzebę narzędzi, które nie tylko usystematyzują prace, lecz również usprawnią procesy i ujednolicą zarządzanie ryzykiem. W takim razie jak dobrze zarządzać procesami klinicznymi, by nie tylko zminimalizować ryzyko kliniczne, lecz również zaoszczędzić? Kilka lat temu rozpoczęliśmy wdrażanie narzędzi lean celem usprawnienia naszej działalności. Obserwując codzienne procesy i wydarzenia z tym związane, zauważyliśmy, że nie zawsze praca jest łatwa, jednolita i bezpieczna. Nasi pacjenci jak i pracownicy korzystali z przestrzeni wspólnych nie mając świadomości, że pewne miejsca powinny być zawsze łatwo dostępne. Nikt z pracowników wcześniej nie słyszał o zarządzaniu wizualnym, na pewno część osób spotkała się z tym, lecz nie była świadoma, że to jest zarządzanie wizualne, sytuacje, które to potwierdzały nie niosły nic dobrego. Czym właściwie jest zarządzanie wizualne? Jest to technika komunikacji, która rozpowszechnia komunikaty do pracowników (komunikaty graficzne, dźwiękowe) bezpośrednio zaangażowanych w proces jak i pośrednio. Pozwala na szybką ocenę stanu aktualnego, która umożliwia szybkie wychwycenie odchyleń. Zarządzanie wizualne pozwala na wykonanie pracy szybciej i zgodnie z określonymi krokami.
VM odpowiada na pytanie: w jaki sposób możemy zaprojektować przestrzeń, która będzie użyteczna i dostosowana do potrzeb uczestników procesu?” oraz stwarza transparentne warunki pracy.
Przedstawienie problemu
- Co się wydarzyło: Procesy zachodzące w RCN nie były optymalnie zarządzane (biorąc pod uwagę fakt, że głównym uczestnikiem procesu był pacjent, należało zwiększyć jego bezpieczeństwo. Przestrzenie pracy były nieuporządkowane, stanowiska częściowo źle rozmieszczone, nie wszystkie zasoby policzone. Organizacja miejsca pracy nie sprzyjała tylko tworzeniu wartości dodanej, ponieważ występowały elementy marnotrawstwa. Kiedy po wdrożeniu normy PN-EN 15224 Usługi sektora ochrony zdrowia, nadal występowały opóźnienia w przygotowaniu stanowisk pracy, często występowały uszkodzenia sprzętu medycznego (takiego jak USG, EKGS, wagi pacjenta), sprzęt był przestawiany z kąta w kąt, co powodowało dodatkowy wysiłek personelu w celu lokalizacji sprzętu i kontroli jego stanu technicznego.
- Gdzie się wydarzyło: Problemy zauważono w RCN, na Sali dializ, w przestrzeniach wspólnych,
w oddziale nefrologii i w poradniach diabetologicznej i nefrologicznej, - Kiedy zostało zidentyfikowane: Bariery i przeszkody, które zidentyfikowano w procesach klinicznych wystąpiły w 2014 roku, w kwietniu.
- Jak długo trwała sytuacja: Sytuacja trwała od 2013 roku.
- Ile jest problemów: Lista problemów zidentyfikowanych w RCN była dość długa i dotyczyła: źle ustawionych wózków inwalidzkich przy drogach komunikacyjnych, nie przypisania stałych miejsc odkładczych dla sprzętu medycznego takiego jak USG, EKG, wagi siedzące i stojące, wózki inwalidzkie, poszukiwanie sprzętów i materiałów jednorazowych oraz do mycia, które znajdowały się w kilku różnych magazynach, przeterminowane leki, wysoki poziom zapasów leków, materiałów jednorazowych i sprzętu medycznego, zmęczenie pielęgniarek i salowych, przez szukanie zasobów do pracy, dodatkowe liczenie zapasów w magazynie, niejednolity proces kliniczny. Te wszystkie utrudnienia powodowały dodatkową frustrację personelu oraz obniżały poziom jakości pracy. Podsumowując zidentyfikowano występowanie sześciu następujących marnotrawstw, zgodnie z filozofią lean:
- Nadmierny ruch,
- Nadmierny transport,
- Zapasy,
- Oczekiwanie,
- Błędy,
- Nadprocesowość
- Jakiej populacji dotyczy problem: Problem opisany powyżej dotyczył całego personelu medycznego w RCN, zarówno pielęgniarek, lekarzy, salowych, osób zarządzających jak
i pacjentów. Problemy zlokalizowano w dwóch jednostkach medycznych (Miastko i Szczecinek) - Kogo dotyczy problem: Trudności występujące w codziennej pracy RCN dotykały właścicieli procesów, ich uczestników oraz osób wspomagających procesy. Przedstawiając dane w liczbach ma się to następująco: problem dotyczył
- 52 pracowników
- 64 pacjentów dializowanych,
- 300 pacjentów hospitalizowanych,
- 1200 pacjentów korzystających z poradni w odniesieniu do roku pracy.
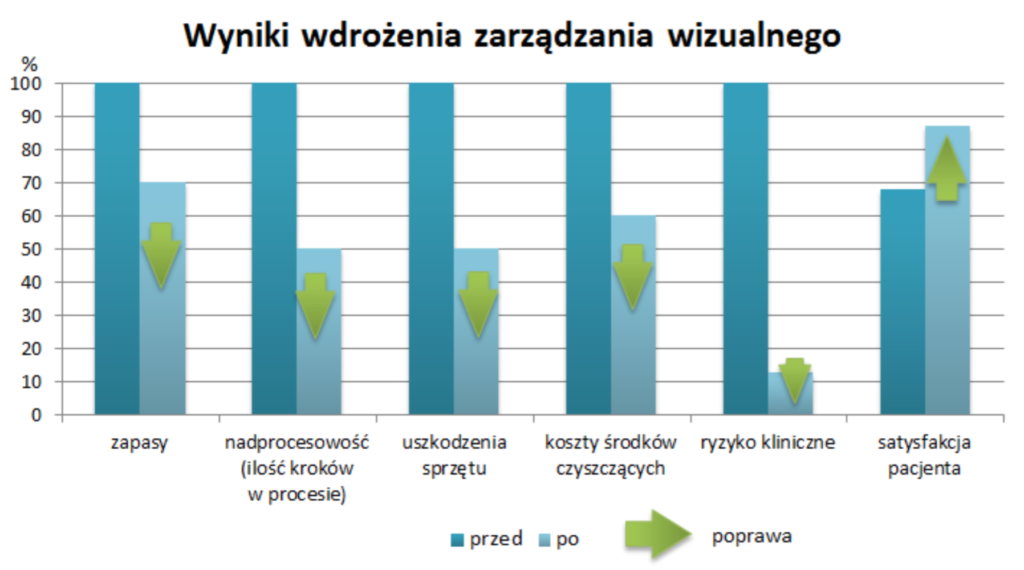
Wykres 1: Wyniki wdrożenia zarządzania wizualnego w Regionalnym Centrum Nefrologii w Polsce, źródło: opracowanie własne
Wykres 1 przedstawia wyniki jakie uzyskano we wskaźnikach RCN po wdrożeniu narzędzi dotyczących zarządzania wizualnego. Dzięki zastosowaniu kart kanban, które usprawniły przepływy w magazynach, identyfikację produktów oraz utrzymywanie zapasów na bezpiecznym i optymalnym poziomie udało się zmniejszyć ilość magazynowanych leków i sprzętu medycznego o 30% w odniesieniu rocznym. To przełożyło się na spore oszczędności finansowe, które można wykorzystać na inwestycje. Warto również wspomnieć o poprawie stosowania metody FEFO (pierwsze traci ważność, pierwsze jest wykorzystywane) co wpłynęło na zmniejszenie leków przeterminowanych. Stosując flowcharty głównych procesów klinicznych zmniejszono ilość czynności, które były niepotrzebnie realizowane lub powtarzane. Pozwoliło to na skrócenie procesu leczenia pacjenta, standaryzację procesu i lepszy przepływ informacji. To poprawiło czas taktu (czas taktu mówi nam co jaki czas powinno być realizowane zamówienie klienta, mając dostępny określony czas np. 8h-1 zmianę; jest to stosunek ilości zamówień klienta do dostępnego czasu, wynikiem jest wskaźnik, który określa w jakim czasie 1 zlecenie klienta powinno być zrealizowane by w odniesieniu do np. 1 zmiany wykonać zlecenia klienta przewidziane na 1 zmianę). Zwięzłe i czytelne diagramy zachęciły personel do korzystania z mapy procesu zwiększając przy tym bezpieczeństwo. Wdrożenia narzędzia proces flow diagram zmniejszyło nadprocesowość o 50%.
Po akcji oklejenia miejsc odkładczych dla sprzętu medycznego ilość uszkodzeń drogiego sprzętu zmalała o 50%, co wpłynęło na poprawę bezpieczeństwa realizacji usług oraz zapewnienie ciągłości procesu. Przykładem nadprocesowości są również niestabilne procesy kliniczne, które przez różnych lekarzy były wykonywane na inne sposoby (to wydłużało proces, dodając zbędne czynności). Koszty środków myjących i czyszczących zmniejszyły się o 40% ze względu na rozdział pomieszczeń gospodarczych i przyporządkowanie ustalonej ilości środków dla każdego piętra (3 i 5 piętro firmy).
Odnosząc się do ryzyk związanych z procesami klinicznymi poniżej w Tabeli nr 1 przedstawiono próbkę z analizy FMEA, która została wykonana w RCN dla procesu hemodializy oraz hospitalizacji w oddziale nefrologicznym. Pamiętajmy, że analiza FMEA dotyczy przyczyn i skutków potencjalnych błędów- jest to szacowanie ryzyka, które może wystąpić w przyszłości. Występowanie wysokiego ryzyka w procesach powoduje wiele problemów, lecz również wydłuża proces, co powoduje zwiększenie kosztów hospitalizacji pacjenta. Największa poprawa wskaźnika RPN dotyczy zakażeń pacjenta w oddziale nefrologicznym.
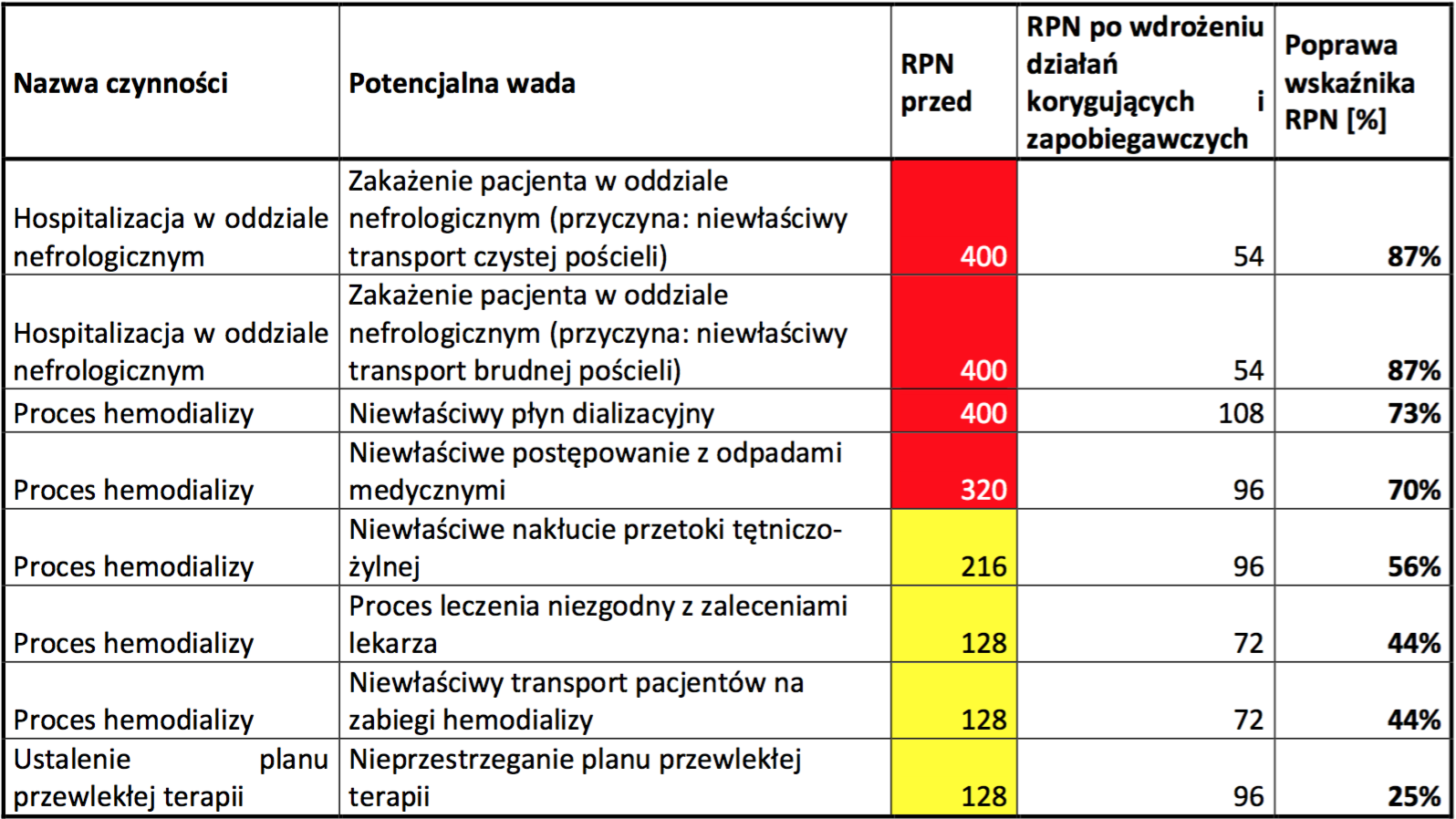
Tabela 1: Część analizy FMEA dla procesu Hospitalizacji pacjenta w oddziale nefrologicznym oraz procesu Hemodializy w Regionalnym Centrum Nefrologii, źródło: opracowanie własne
Początek
Pierwszym krokiem była analiza obecnego stanu, urządzeń i pomieszczeń. Oceniono czy urządzenia medyczne znajdują się w pomieszczeniach, w których są wykorzystywane czy może za każdym razem trzeba je przestawiać lub przenosić na duże odległości. W pomieszczeniach sprawdzono dostępność rzeczy, które są niezbędne do pracy.
Czy technika optymalizacji procesów stosowana w przemyśle motoryzacyjnym może być zaadoptowana w szpitalach? Otóż procesy, które wzajemnie na siebie oddziałują tworzą wartość dodaną, generując przy tym koszty działalności. Istnieje „lek”, który może zwiększyć wartość dodaną i obniżyć wydatki. Ratunkiem jest filozofia lean management, która przy wykorzystaniu odpowiednich metod i narzędzi eliminuje zbędne czynności i straty (czasowe, finansowe, zasobów) zwiększając jakość, bezpieczeństwo i efektywność procesów (przy zmniejszaniu kosztów ich realizacji). Zwraca uwagę na wskaźnik jakości, oczekiwania, przepływy pacjentów, spójność komunikatów, odpowiedni system znaków informacyjnych i przebieg procesu.
Realizując kaizenową drogę od marnotrawstwa po samą wartość dodaną, bardzo ważnym elementem była komunikacja. Nie jest to nic odkrywczego, a miało znaczący wpływ na projekt. Zespół medyczny początkowo nie był przychylny wprowadzaniu nowych metod i zmian ze względu na nieznane dotąd nazewnictwo wszystkich technik i narzędzi lean. Biorąc to pod uwagę dostosowano poziom słownictwa i komunikaty do uczestników. Mówiąc o narzędziach lean, szkoląc, organizując warsztaty nazywano narzędzia ze względu na ich cel (nie 5s ale uporządkowane miejsce pracy, nie flowchart ale ścieżka postępowania w leczeniu). To zachęciło uczestników do aktywności i dzielenia się swoimi uwagami i pomysłami.
Inwestycje
Kolejnym krokiem były spotkania i narady pracowników (pielęgniarki, lekarze, salowe, inżynier lean hospitals) w celu przedstawienia narzędzi lean, które mogą być wdrożone, przedstawiono każde z nich w praktyce, również dzieląc się praktycznymi przykładami z innych jednostek medycznych ochrony zdrowia. Po prezentacji zespół przeszedł do burzy mózgów, która była krokiem milowym w stworzenia planu wdrażania narzędzi VM. Zespół zebrał pomysły, które dotyczyły miejsc i aspektów do poprawy, do zastosowania narzędzi i metod lean management. Praca była szybka i entuzjastyczna, rozpalała kreatywność personelu do tego stopnia, że wybrano zestaw narzędzi, które zdecydowano się zastosować w codziennej pracy RCN.
Na kolejnym etapie projektu, opracowano proces flowchart diagram dla 7 głównych procesów zachodzących w RCN:
I. terapia nerkozastępcza – hemodializa,
II. terapia nerkozastępcza – dializa otrzewnowa,
III. porada nefrologiczna,
IV. porada diabetologiczna,
V. hospitalizacja w oddziale nefrologicznym,
VI. proces leczenia niedokrwistości w predializie,
VII. leczenie nadczynności przytarczyc u osób hemodializowanych.
Lean zapewnia powtarzalność realizacji usług, poprawia stabilność procesu i utrzymuje odpowiedni poziom jakości usług w planowaniu długoterminowym. Zaprojektowano znaki poziome na podłogi, z przeznaczeniem na miejsca odkładcze dla sprzętu medycznego (łóżka, wózki inwalidzkie, fotele, wagi, USG, EKG, sprzęt do sprzątania, stoliki, miejsca dezynfekcji rąk). Zakupiono żółte znaki informacyjne o mokrej podłodze, zakupiono taśmę czerwoną i żółtą do wydzielenia pól odkładczych i poziomu zapasu bezpieczeństwa w magazynach. Ustalono podział kolorów na poszczególne stanowiska dla personelu oraz stworzono karty kanban dla magazynu.
Postanowiono zastosować:
- 5S
- flowcharty dla procesów głównych
- wizualizacja miejsc odkładczych,
- organizacja dokumentacji jakościowej,
- zastosowanie różnych kolorów uniformów dla personelu medycznego,
- standaryzacja kolorów sprzętu do sprzątania.
Koszty powyższych aktywności zostały przedstawione w tabeli 2

Tabela 2: Koszty inwestycji w Regionalnym Centrum Nefrologii w Polsce, źródło: opracowanie Douglas C. Wood, Katarzyna Złotowska
Monitorowanie
Po wdrożeniu wybranych narzędzi lean należało monitorować efekty. Pracownicy byli świadomi, że praca według filozofii lean nie polega na jednorazowym wdrożeniu rozwiązania , podstawą tych technik jest ciągłe doskonalenie, ponieważ ludzie nie popełniają celowo błędów, tylko procesy są źle zorganizowane. Salowe każdego dnia pracy na koniec zmiany oceniają zgodnie z metodologią 5S stan pomieszczeń i infrastruktury w RCN. Dlaczego salowe? Ponieważ to one codziennie mają dostęp do większości pomieszczeń w RCN, są osobami rzetelnymi i sumiennymi, wiedzą, że ich praca ma duży wpływ na bezpieczeństwo pacjentów. Ocenę wykonują na specjalnie stworzonym arkuszu oceny 5S, który został przystosowany do organizacji pracy jaka funkcjonuje w RCN. Salowe oceniają nie tylko ład i porządek, lecz również stan techniczny (ogólny) infrastruktury i efekty swojej pracy w czasie rzeczywistym. To im zajmuje średnio 10 minut dziennie. Co tydzień tablica wizualna ze wskaźnikami jakościowymi jest uzupełniana przez inżyniera lean hospitals. Dane są prezentowane w sposób przejrzysty, zrozumiały i dostępny dla całego personelu. Pozwala to na szybką ocenę procesów w organizacji.
Zatem czy codzienne oceny wystarczają? W celu otrzymywania odpowiedzi od osób odpowiedzialnych za ocenę 5S, prowadzone są audity 5S przez inżyniera jakości-lean hospitals. Pozwalają one na zebranie nie tylko oceny, która jest pozytywna, również na zebranie tematów, które należy omówić i rozwiązać. 5S buduje jakość, jak mawiał Henry Ford, „Jakość oznacza robienie rzeczy dobrze gdy nikt nie patrzy” i tak też pracują nasze salowe.
Każdy kwartał roku owocuje zmianami, usprawnieniami procesów, które są analizowane przez wszystkich, i przedstawiane na spotkaniach jakości przez osoby znajdujące się w zespole ds. jakości. Jest to praca twórcza w oparciu o gemba walk, wywiady bezpośrednie z uczestnikami procesów oraz personelem medycznym.
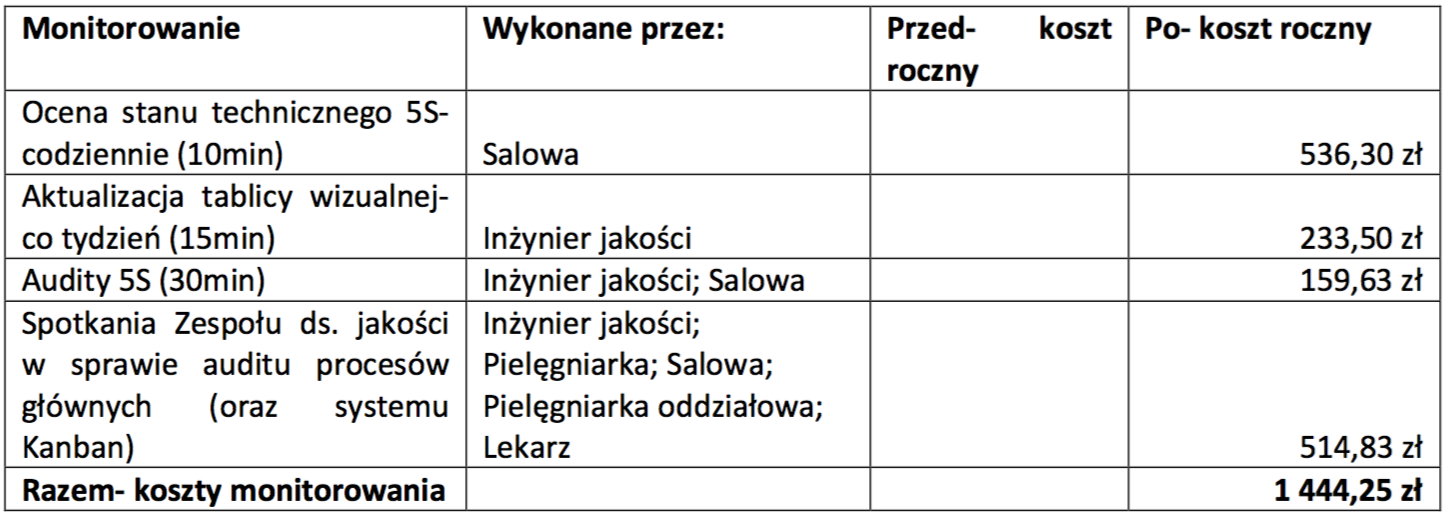
Tabela 3: Koszty monitorowania w Regionalnym Centrum Nefrologii w Polsce, źródło: opracowanie Douglas C. Wood, Katarzyna Złotowska
Wewnętrzne marnotrawstwo
Czym jest marnotrawstwo? Są to wszelkie czynności i operacje, które nie dodają wartości do procesu, wydłużają proces, a za które pacjent i płatnik czyli NFZ nie chce płacić. Jakie więc marnotrawstwa (muda) zidentyfikowano w RCN?
- Zbędny ruch pielęgniarek. Podczas zabiegów hemodializ lub opieki nad pacjentem w oddziale pielęgniarki często musiały szukać materiałów potrzebnych do wykonania zabiegu. Szukały go nie tylko w sali dializ, również w magazynach, które są zlokalizowane na 2 piętrach, a w których materiały mogły się powtarzać. Należy zauważyć, że to powodowało nie tylko zmęczenie personelu, również stracony czas, zaniżony poziom bezpieczeństwa pacjenta, brak skupienia się na procesie.
- Zapasy leków, materiałów jednorazowych i sprzętów w magazynach. Zapasy to „zamrożony” kapitał, który mógłby być wykorzystany na realne usprawnienia. Kumulacja zamówień, czasami tych samych, zamawianie towarów, które znajdują się na stanie (zazwyczaj w kilku różnych miejscach), problemy z inwenturą i straty finansowe wynikające z przeterminowanych leków. Procesy medyczne są specyficzne i nie da się określić precyzyjnego popytu na nie, lecz można to oszacować na podstawie miesięcznych wyników, dodając małą nadwyżkę, tzw. zapas bezpieczeństwa, który zapewni nam ciągłość procesu klinicznego.
- Braki, odnosząc się do RCN były to uszkodzenia sprzętu, powodowane zbyt częstym przestawianiem, niezgodnym użytkowaniem i brakiem określonych lokalizacji „adresów” tych przedmiotów.
- Nadprocesowość, czyli wykonywanie czynności zbędnych, takich jak częste zamawianie towarów do magazynu szpitala. Mając różne magazyny, nieporządek i brak potwierdzonych ilości zamawianie towarów przez oddziałową odbywało się 4 razy w miesiącu.

Tabela 4: Koszty wewnętrznego marnotrawstwa w Regionalny Centrum Nefrologii w Polsce, źródło: opracowanie Douglas C. Wood, Katarzyna Złotowska
Konsekwencje
Oceniając i analizując procesy wyszczególniono kilka potencjalnych konsekwencji, które mogą przyczynić się do wzrostu czynności nie przynoszących wartości dodanej, negatywnych skutków i obniżenia poziomu jakości usług medycznych w RCN. Według salowych istnieje możliwość nie użycia znaków
do mokrej podłogi , według pielęgniarek i lekarzy ryzykiem jest nie przestrzeganie wewnętrznych procedur i instrukcji, w tym flowchartów.
To co najważniejsze i co napędza procesy medyczne to pacjent. Pacjent jest najważniejszym „elementem” procesu, który rozpoczyna i kończy proces. Dla RCN każdy proces musi przynosić wartość dodaną dla pacjenta, ryzykiem nieprzestrzegania polityki RCN, misji jest obniżenie satysfakcji pacjentów, zwiększenie ilości skarg. Jak wspomniano na początku pacjent obserwuje czy zabieg został wykonany na czas, czy środowisko w którym jest leczony jest przyjazne, czyste i bezpieczne. To tworzy całokształt działań związanych z lean hospitals –lean healthcare.
Zwrot z inwestycji
Dokonując porównania kosztów realizacji procesów w RCN przed i po wdrożeniu narzędzi lean management, lean healthcare określono oszczędności jakie uzyskano. W sumie w ujęciu rocznym RCN uzyskało 61 833,62 zł oszczędności realizacji procesów dzięki stosowaniu zarządzania wizualnego. Stosunek oszczędności do nakładów wynosi 15,6:1.
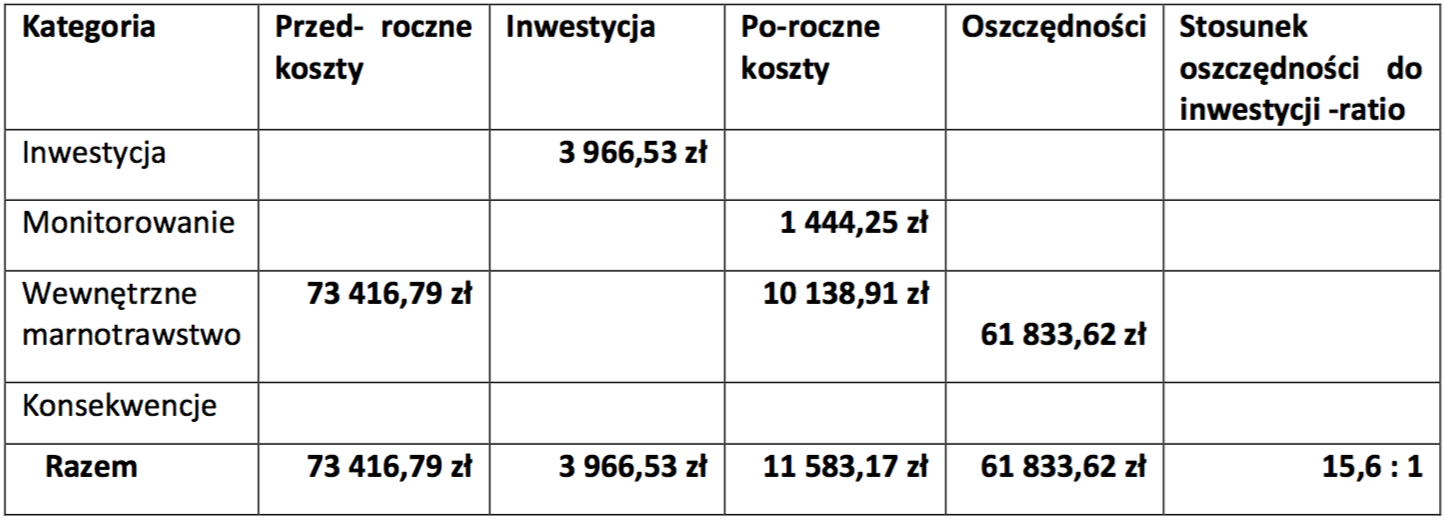
Tabela 5 : Podsumowanie kosztów dla Regionalnego Centrum Nefrologii w Polsce, źródło: opracowanie Douglas C. Wood, Katarzyna Złotowska
Wyniki i kolejne kroki
Najważniejszą rzeczą w komunikacji jest by słyszeć to co nie zostało powiedziane, Peter Drucker…i by dostrzegać to czego nie widzą inni..
Podsumowując zarządzanie wizualne ma ogromny wpływ na koszty jakości. Jest ono istotnym elementem komunikacji. Personel medyczny podejmując się opieki nad pacjentem bierze na siebie odpowiedzialność, nie tylko za technikę pracy, lecz również za poprawę jakości życia pacjenta. Wszelkie słowa, gesty, materiały pisane i audiowizualne poprawiają komunikację i cały proces leczenia. Dostosowanie poziomu zarządzania wizualnego do różnych potrzeb i sytuacji sprawia, że pacjent czuje się bezpiecznie, a pielęgniarka pewnie siebie.
Jakie są kolejne kroki RCN w budowaniu organizacji opartej na zasadach i narzędziach lean management oraz dbającej o koszty? Jako organizacja nowoczesna, w której centralnym elementem jest pacjent, planuje wdrożyć kolejne narzędzia lean management dostosowując je do zadań i pracy oraz możliwości pracowników. Obecnie wdrażany jest model rozwiązywania problemów oparty na formularzu A3. W kwietniu 2016 odbyło się szkolenie praktyczne na przykładzie problemów, które zebrano od pacjentów i pracowników RCN. Mówiąc o ciągłym doskonaleniu, obecnie wdrażane jest 5S u lekarzy w gabinecie lekarskim.
Należy pamiętać, że projekt nie dotyczył wszystkich procesów występujących w RCN i wyniki jakie zostały przedstawione odnoszą się do małego szpitala. Wartości poszczególnych sekcji (inwestycja, monitorowanie, wewnętrzne marnotrawstwo i konsekwencje) obliczono na podstawie mediany pensji w dolarach amerykańskich z I kwartału 2016. Zastosowano wskaźnik wartości siły nabywczej dla Polski za rok 2015. Dane pobrano z www.stats.oecd.org
To co jest zaplanowane na rok 2016 to poprawa komunikacji interpersonalnej, główny punkt tego projektu to komunikacja na linii pacjent-pielęgniarka, lekarz-pielęgniarka, lekarz-pacjent. Optymalizacja procesów klinicznych i organizacja sali operacyjnej zgodnie z zasadami lean. Zaplanowano remont i rozbudowę infrastruktury. Na podstawie analizy FMEA procesu hemodializy, dializy otrzewnowej, hospitalizacji pacjentów w oddziale nefrologicznym aktualnie usprawniane są procesy, procedury i flowcharty, itp.
Rok 2016 jest rokiem ważnym dla RCN, ponieważ organizacja przygotowuje się do tranzycji SZJ opartego na wymaganiach normy ISO 9001:2015 nowej wersji.
Bibliografia
- Łazicki A. i in. Systemy zarządzania przedsiębiorstwem-lean management i kaizen, Wiedza i Praktyka, Warszawa 2011
- Locher D., Lean w biurze i usługach, tłum.Gasper D., MT Biznes, Warszawa 2012
- Wruk-Złotowska A., Komunikacja pomiędzy pacjentem a pielęgniarką jako element bezpieczeństwa procesów klinicznych, Medical Maestro

Katarzyna Złotowska MBA
Ekspert lean healthcare, inżynier ds. optymalizacji procesów klinicznych, właściciel LH, audytor wiodący ISO (rej. W IRCA), trener, six sigma green belt, autor książki.

Douglas C. Wood
Prezes firmy konsultingowej DC Wood Consulting, LLC, członek Amerykańskiego Stowarzyszenia Jakości ASQ, wydział Zarządzania Jakością. Współpracuje z klientami z branży produkcyjnej i medycznej. Posiada ponad 30 lat doświadczenia w inżynierii przemysłowej i jakości.
Wszelkie kopiowanie, zmiana treści bez zgody autora, nie podając źródła jest zabronione. Copyright by LeanHospitals
Communication with patient
Working in healthcare consists of numerous relations with patients, their families and close relatives. Work is stressful and includes difficult requirements and situations. Communication in clinical processes is essential for medical services. Communication is strictly connected with treatment results and as an essential factor and it is important to make it as smooth, uninterrupted and flawless. Communication can be verbal and nonverbal. Today there is a lot of communication methods. Modern and intelligent technology allows for fast, legible contact but is it understandable? Is everything what I say coherent for listener?
Communication is also a kind of behaviour. Last my observations, while I was standing in queue to registration in hospital, shows that it is not so easy. Patient is not easy customer, wants everything fast, no queue, no waiting, without any good manners. I think that situation in which person is a patient, use medical services, is not in comfortable situation. This people are helpless and stressed. We cannot accept anger but we should try to understand them. There is 4 type of patients:
Unaware patient doesn’t think about symptoms and physicians recommendation . Put off visit and try to cure by themselves. We should educate this patient.
Neutral patient talk small, no react, could be paralyzed because of fear, maybe powerless? You as physician, nurse or secretary should be open minded and kind, explain calmly all recommendations.
Patient which lay claims to hospital has got excessive expectations, can be oversensitive. Conversation with that type of patient could be long and not nice.
An arrogant patient could be agressive patient. Is full of pretensions and regrets. The best solution is not to discuss, better is stay calm, ignoring all quarrel.
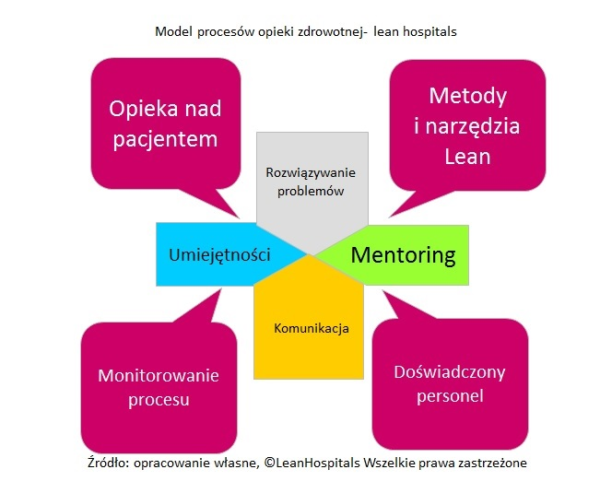
Patient doesn’t has just rights but also duties, one of them is cultural behavior. Below is presented model of healthcare processes- lean hospitals, in which communication is one of the most important elements in good conducted service.
Why we meet conflicts every day in medical life, between patients and medical personnel? The root cause is wrong communication 2 people on different personality states. Each state is characterised different behaviour.
When two persons talk to each other, being on different personality states, don’t understand each other, conflict is next step. There are 3 types of states: I as parent, I as child, I as adult. Good communication makes easier clinical process optimization.
Interview about lean healthcare
I’m glad to share with you an interview about lean management process in polish healthcare. Lean heathcare is a philosophy that not only improves work, but also change the way of thinking person who participate there.
Here you can listen to interview
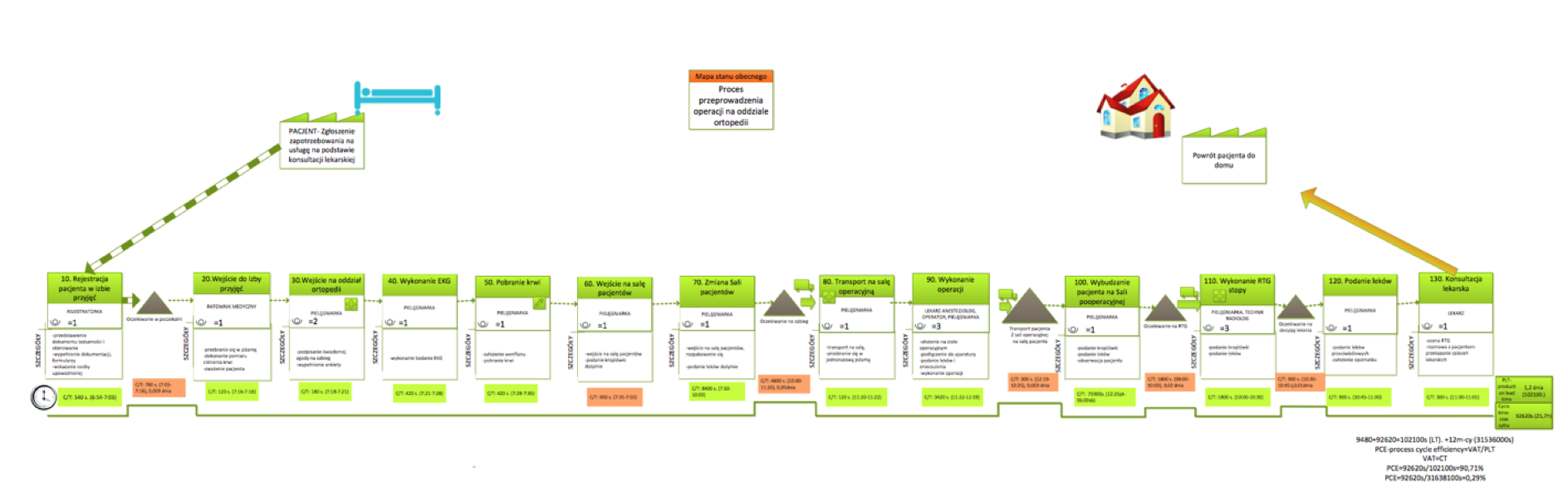
Value stream mapping of a healthcare process
How to map a process?
How can we know the process in which we are participants or owners and have big influence for its efficiency? Sometimes we are not aware how detailes is the process and how many factors affects for realization. If we want to analyze in details the process, know strenghts and weak side we should go to GEMBA. It is real place of process.
VSM is divided into 4 steps
- Draw main flowchart with bigger steps.
- Draw value stream map with details.
- Conduct analysis and prepare future state map.
- Implement changes and do continuous improvement.
Process improvement using value stream mapping
Value stream mapping let us to prepare “road map” for process participants in medical unit. Tool is to spread out the prime factors and analysis each steps. The process is divide on activities that gives values, thanks to that patients receive what they need and activities, which doesn’t give value but has to be present and also in the process are activities which could be eliminated because doesn’t give value, it is 8 types of wastes:
- Motion
- Transport
- Waiting
- Over-processing
- Inventory
- Mistakes
- Over-production
- Wasted human potential
Lean healthcare use this tool in order to know better process, collect all relevant data and eliminate wastes. Based on current state is possible to find out weak points that can be improved. Sometimes analysis can be activated after serious problem occurred, sometimes it could be top management initiative or willingness to implement lean hospitals philosophy.
Key features of value stream mapping
- Process optimization
- Clinical risk analysis
- Time reduction for medical activities
- Descrease processes costs
- Elimination bottlenecks
- Create new standard for process – procedure
- Decrease quantity of adverse events, medical mistakes and nonconformities
Sustaining defined standards for process let us to find out immediately every mistake and deviation so we can react fast and eliminate them.
During preparation value stream mapping we should know the process and have relevant information. Then would be possible to eliminate bottlenecks and muda. The very important thing is to define sequence of steps, participants as physicians, nurses, technicians. For every activity we should measure the time of duration. Based on this values would be possible to define Process Cycle Efficiency.
Value stream mapping takes some time and then we can find out bottlenecks. The bottleneck is point in process which cannot recycle given elements in specific time, so queue are presents. It is a place with the lowest productivity.
Visual management
Visualization tool which allow to quickly and easily identify information such as:
- method and organization of the process
- Value added in the whole process and its parts
- Loss / muda (not value added) – based primarily on 8 losses.
- Information influencing and resulting from the process
- Frequency of information
- Type of information (kanban, verbal information, electronic information, instructions, etc.)
- Process tact
- Time and material buffers
- Quantity per unit of measure (number of pieces, seconds, etc.)
- Quantity of human resources in a current process
One of the objectives of the mapping of the value stream is to create a current state map that is currently running in the facility. It shows dependencies and information that are included in the service process. Then create a future state map, ie develop a process that will satisfy the patient and the worker, will reduce the time or cost of work that means it will reach the planned goals.
Each subprocess contains the C / T (time cycle) information which is the actual execution time of the activities that consist of subprocess, L / T (lead time) which is period starting from the time the patient enters the dialysis room to the return to the home by patient and T / T (tact time) is theoretical execution time of the subprocess.
Methodology consists the creation of current and future state maps, three measures of time of two processes and averaging these times. All actions don’t occur after each other, some of them can be executed at the same time.
Lean Management at healthcare conference
At last monday took place conference, that has opened national project “Lean management in health care”, organized by Polish Society of Health Economics in Warsaw-18.04.2016. The main purpose of project is to creation and standarization National Standards for Value Stream Mapping in polish health care.
During conference, there was few presentations about interesting case studies connected with lean management in health care. LeanHospitals also presented case study about visual management project in hospital. We were talking about clinical processes, which in order to optimalize, have to be mapped, described in details, analyzed and define key perfoRmance indicators (KPI) for continuous improvement. Also methodology 5S was interesting topic with practical examples.
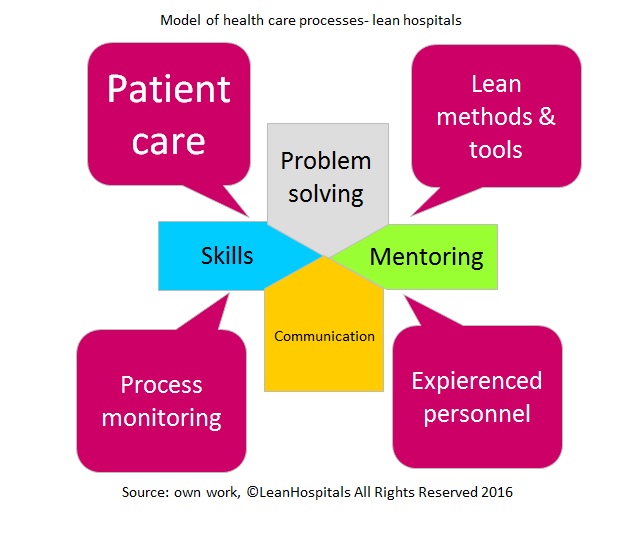
During the conference, I’ve presented 2 models which were created during my project in healthcare in hospital. First model talks about clinical processes in lean healthcare approach. In order to safety process realization important is experIenced medical personnel with qualifications and knowledge. For staff, which is new, mentoring process is important thing. Older and more experIenced colleagues from operating theatre should teach and show the best practices in daily work. Good leader is a person which others follow to, want to cooperate, because they see that leader is open minded, patient and motivating not just commanded. Good team has influence on quality level of treatment process.Patient is main “element” in the process, in which are problems. They should be analyzed and eliminated. Before we will find good solution, we should take deep breathe and understand the problem. Not always thoughts in patient mind are well understood. When we fail in this step, we will take wrong corrective actions, which won’t give you positive results. Also we should use lean management tools as 5why, Pareto, Ishikawa diagram, FMEA etc. When we know well the process, we can every day enhances it. In complete model good communication is an aspect that ensures smoothly process flow. Thanks to that level of safety processes is high, we can improve them and adapt to patient expectations, which won’t make worse effectiveness.
Below I’m presenting Model of health care processes in lean hospitals approach
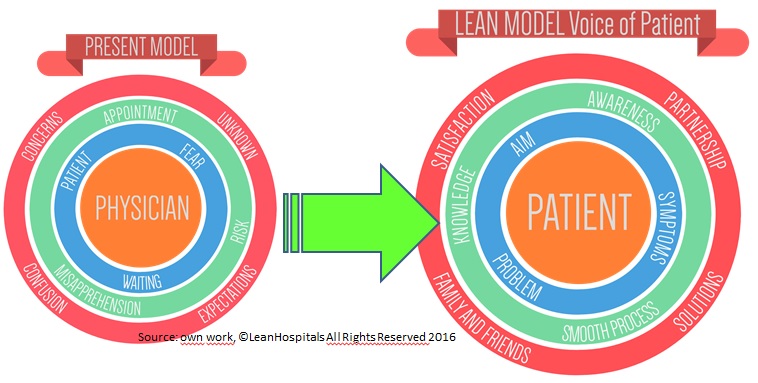
Next model, which I’ve created during projects is Model of patient relation in clinical process in lean hospitals structure.
I show you actual model, in which physician is in the middle of treatment process. Patient, which also is involved has hinder availability to physician, is confused and frightened. He feels alone in the process, without any support. This patient is waiting for new treatment or next step in this treatment. Sometimes an appointment has got risks, that patient won’t be good understood, doctor will do correction without eliminating the root cause of the problem, of disease. Of course it’s not always possible because medical service is not homogeneous service, immaterial and unsustainable, so we cannot predict the results in 100%.
The new model I propose is innovative model. This time Patient is in centre of interest for clinical process. Where go patient, there goes “value”.Patient come in to hospital with problem and purpose. Also this type of patient has got some fear but is aware about his disease and well educated. With respect to that he take active part in clinical process, in which he smoothly flow from one step to the next step, using lean management tools and approach. Based on partnership cooperation physician with patient and his family, some solutions are defined, so the patient feels better, is pleased and feel co-responsible for treatment.
Polish hospital as the best case study of Lean Enterprise
As Project Manager I was awarded the prize for Regional Nephrology Centre as one of the best lean project in healthcare in Poland.
Project was evaluated by the best experts of lean:
Mike Orzen
Chris Vogel
Samuel Obara

GEMBA walk
How can you be sure that something works correct? Sitting in your cosy chair in your office doesn’t make you sure that clinical processes are conform. As doctor’s everyday do doctor’s round, so you can do the same and go where clinical processes are going on, where you can meet medical staff, talk with physicians, patients, technicians. By this way you will know much more that just working in your office. Don’t be afraid, you will win, because more information you can capture observing real processes than calculate it in excel file. For example you can check if 5S methodology works (for more information about that click here). GEMBA walk is one of few tool used in lean hospitals, lean healthcare philosophy.